Best types of creatine to take: Absorption, benefits, and is it worth paying more?
By: Andrew Forrest - January 2026
Confused by creatine types? Evidence-based UK guide to the best types of creatine to take, absorption, dosing (3-5g), safety, and whether expensive forms are worth it.
Table of contents
This page contains affiliate links. If you buy products or services via these links, we may earn a small commission at no cost to you. If you are thinking of buying, please use our links, as it helps support our website and YouTube channel.
Creatine is also one of the most extensively researched supplements, with evidence supporting improvements in strength, power, repeated
high-intensity performance, and training adaptations when paired with exercise. It's not just for bodybuilders.
Walkers, hikers, and everyday active people can benefit most when their routine includes hills, intervals, gym work, or carrying loads. This
guide breaks down what actually works (and what's mostly marketing), explains how to dose creatine simply, and helps choose a product without
overpaying - with safety considerations for people who may need extra caution.[1] [2] [11] [12] [33] [34]
Health & Wellness Disclaimer
The information in this article is intended for general education and wellbeing and discusses creatine supplementation, including potential
benefits, dosing approaches, product selection, and safety considerations for generally healthy adults.
Creatine may not be suitable for everyone. If you have any medical conditions - especially kidney disease or reduced kidney function, high or
unexplained creatinine blood results, liver disease, hypertension, or any long-term condition - or if you are pregnant or breastfeeding, under
18, have a history of bipolar disorder, or are taking prescription medicines (particularly those that may affect kidney function), you should
speak to your GP, pharmacist, or another qualified healthcare professional before starting creatine or changing your supplement routine. If you
have been advised to limit protein, fluids, or certain supplements for medical reasons, do not start creatine without professional advice.
This article does not provide medical advice and should not be used as a substitute for professional healthcare. Supplements are not regulated
in the same way as medicines in the UK, and product quality can vary between brands. Always follow the manufacturer's directions, do not exceed
recommended doses, and stop use and seek medical advice if you experience concerning symptoms. If you develop urgent symptoms such as chest
pain, a severe allergic reaction, fainting, severe vomiting, or signs of acute illness, seek immediate medical attention by calling 999 or
attending A&E.
Creatine is a naturally occurring compound your body produces. You also obtain small amounts from foods such as red meat and fish. Supplementing
with creatine increases muscle creatine stores beyond what most diets provide, which is why it consistently shows performance benefits in
well-controlled research.[1] [3] [4] [5]
Key takeaway
If you want the best type of creatine to take, the evidence overwhelmingly supports:
- Creatine monohydrate (powder or capsules) as the default choice[1] [2] [37] [38]
- 3-5 g daily as a simple, effective dose[1] [2] [5]
- A loading phase is optional (helps you feel the benefits sooner, but is not required)[1] [5]
- Paying extra for advanced forms is rarely worthwhile: most have limited or no evidence of superior outcomes and often cost more[35 ‑ 38)]
Overview
Creatine is one of the most widely studied performance and health supplements. It's widely used for strength, power, repeated high-intensity
efforts, and to support training adaptations[1] [11].
Emerging research also supports potential benefits in healthy ageing, brain energy demands, and certain clinical contexts[1] [25 ‑ 31] - but it's still important to keep expectations realistic and match creatine to the type of activity you actually do.
If you're a walker, hiker, or general fitness trainer, creatine can still make sense: it's most useful when your walking life includes hill
climbs, interval sessions, gym work, carrying loads, repeated sprints, or anything that feels like short bursts of hard effort rather than steady
plodding.[7 ‑ 10]
Basics
What is creatine?
Creatine
is a naturally occurring compound derived from amino acids and stored mainly in muscle tissue (it is also present in the brain). In muscle, it
exists as free creatine and phosphocreatine, acting as a rapidly available energy buffer[3] [4] [5].
Creatine in your muscles exists in two usable forms: 'free' creatine (ready to be converted to phosphocreatine) and phosphocreatine (creatine
with an extra phosphate attached that your body can quickly use to help 'recharge' energy during short, hard efforts).
You can obtain creatine from food (especially meat and fish), but typical dietary intake is far below the amounts used in most research and
supplementation protocols[1] [3].
Should I take creatine supplements?
Creatine is most likely to be worth it if you want at least one of the following:
- More strength/power in the gym[1] [11] [12]
- Better performance in repeated bursts (e.g., hills, sprints, hard intervals, team sports)[7 ‑ 10]
- Support for training volume and adaptation over time[11] [12]
- Help maintain or build muscle as you age[17 ‑ 22]
- Potential support for certain aspects of cognitive performance under stress[26] [27] [28]
The idea of helping maintain or build muscle as you age is interesting to me, as more and more recent studies are linking muscle to longevity.
If your only exercise is long, steady, low-intensity walking, creatine may still help indirectly (e.g., by improving recovery from the strength
work you add in), but it's not a magic endurance pill. Some studies show little or no benefit for pure endurance performance without a
high-intensity component[11].
How creatine works
How does creatine work in the body?
During short, intense efforts, your body rapidly uses ATP. ATP (adenosine triphosphate) is your body's 'immediate energy' molecule - the fuel
your cells use to power muscle contractions and other work, especially during short, high-intensity bursts. The phosphocreatine system helps
regenerate ATP quickly, helping you maintain force and power output for a little longer and repeat hard efforts with less drop-off[3] [4] [5] [7 ‑ 10].
Supplementation raises your muscle creatine stores[4] [5],
which is why creatine reliably benefits high-intensity, repeated efforts more than slow, steady-state exercise.
Absorption and bioavailability of creatine
Creatine monohydrate is well absorbed and effective at increasing muscle creatine[1] [4] [5] [6].
Many new forms claim better absorption, but the key question is: do they outperform monohydrate in outcomes? The best overall evidence suggests:
generally no[1] [35 ‑ 38].
Proven benefits and uses of creatine
Creatine is best known for improving:
- Repeated sprint / repeated high-intensity performance[7 ‑ 10]
- Maximal efforts and high-intensity work capacity[7 ‑ 11]
This is why creatine is so relevant to sports and sessions involving repeated, hard bursts (intervals, hill repeats, circuits, gym work and
certain team sports).
Increasing muscle mass and strength
Across many studies and meta-analyses, creatine supplementation combined with resistance training tends to increase lean mass and strength more
than resistance training alone[1] [11] [12].
Women benefit too. Trials in women show that creatine improves strength and training progress[12] [13].
Muscle recovery and soreness
Creatine may support recovery from hard eccentric work (think downhill hiking and gym work, or strength sessions that leave you sore).
Controlled studies show improved recovery of force after muscle-damaging exercise[14].
Healthy ageing and functional performance
Creatine, combined with resistance training, can be particularly useful in older adults for:
- Increasing strength and fat-free mass[17 ‑ 22]
- Improving certain functional performance outcomes (e.g., tasks related to daily living)[18] [20] [21]
A systematic review/meta-analysis supports additional benefits when creatine is added to resistance training in older adults[19].
This is key, as more studies are linking muscle and longevity.
Bone and falls-related factors
Evidence suggests that creatine, when combined with resistance training, may have potential benefits for
bone-related outcomes,
though this is an evolving area and results vary by study design[23] [24].
In practice, creatine is best viewed as a potential support for a broader healthy-ageing plan that includes resistance training, protein,
balance work, and sufficient vitamin D and calcium.
Blood sugar and glucose control
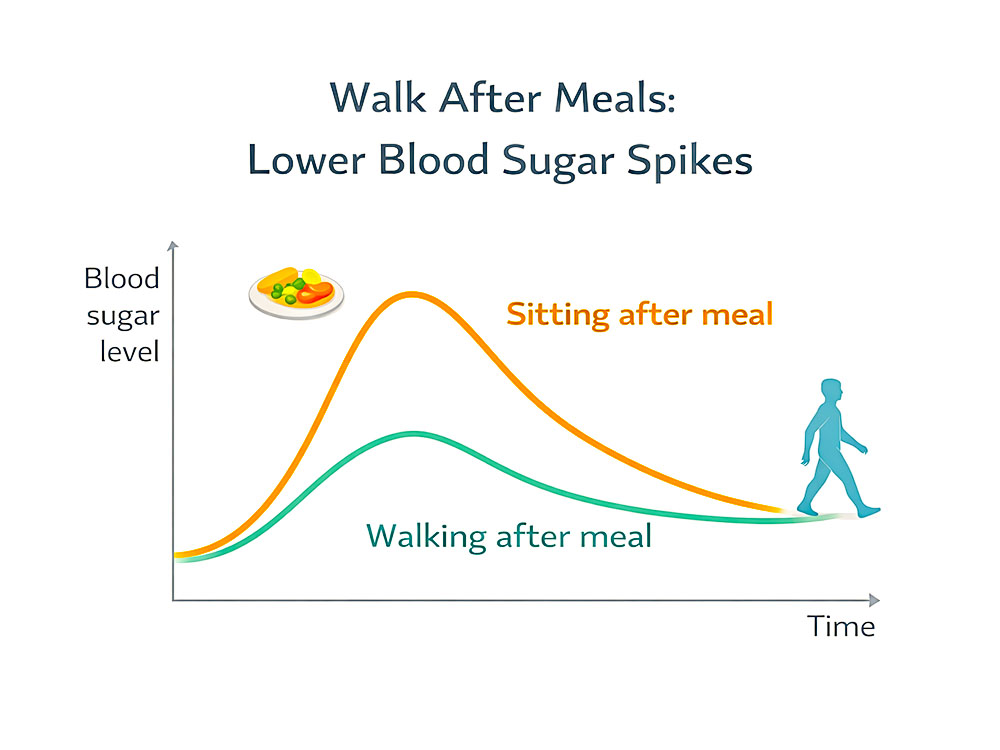
In type 2 diabetes, creatine combined with exercise improved glycaemic control in a randomised controlled trial[25].
This doesn't mean creatine treats diabetes, but it does suggest that creatine may support exercise-mediated metabolic benefits in some
populations[25]. Walking can also
reduce blood sugar spikes.
Brain function and cognition
Creatine plays an energy role in the brain, too[3].
Human trials and systematic reviews suggest potential benefits in certain cognitive domains, particularly under high brain energy-demand
conditions (e.g., stress, sleep deprivation, low dietary creatine intake)[26] [27] [28].
- Improved working memory and reasoning were observed in one controlled trial[26].
- Sleep deprivation studies suggest potential positive effects on mood and tasks that stress executive function[27].
- A systematic review found possible improvements in short-term memory and reasoning, with mixed results across other domains[28].
Mood and mental health
Research has explored creatine as an adjunct in depression:
- An RCT in women with major depressive disorder found that adding creatine to SSRI treatment improved clinical response[29].
- An earlier open-label pilot suggested potential benefit but also highlighted caution in bipolar depression because of the risk of hypomania/mania[30].
This is not a recommendation for self-treatment - it's an area to discuss with a clinician.
Rehabilitation and muscle loss
Creatine has also been studied in rehabilitation contexts. A classic controlled study found that creatine supported rehabilitation from disuse
atrophy and affected markers of muscle regeneration[31].
This matters in real life: illness, injury, immobilisation, and starting again are common.
Types of creatine explained
Creatine monohydrate (recommended)
In my view, this is the gold standard for creatine. It's the form used in the bulk of research and consistently improves outcomes in the
right contexts[1] [2] [11] [37].
Who it suits: almost everyone.
Buffered creatine (e.g., Kre-Alkalyn)
Claims: Fewer side effects, better retention, and a lower dose required.
Evidence: Controlled studies show no meaningful advantage over monohydrate for muscle creatine, body composition, or training outcomes[35].
Unbranded creatine powder and scoop
Creatine ethyl ester
Claims: Better absorption.
Evidence: Controlled research found it was not superior and appeared less effective at raising muscle creatine levels than monohydrate[36].
Creatine HCl, nitrate, magnesium chelate, liquids, blends
These forms are heavily marketed. Independent outcome research is limited, and broader reviews conclude that no alternative form has
convincingly outperformed monohydrate[1] [37] [38].
Walks4all takeaway
If you tolerate monohydrate, as most people do, there's rarely a compelling reason to upgrade.
Absorption & effectiveness of creatine
Usually, no. Across reviews and comparative evidence:
- Monohydrate reliably increases muscle creatine[4] [5] [6]
- Buffered and ethyl ester forms do not show superiority in real-world outcomes[35] [36]
- Broader analyses of marketed alternatives show a pattern of limited evidence and higher cost[37] [38]
Does taking creatine with carbs or protein help?
It can. Studies show that adding carbohydrate (and/or protein + carbohydrate) can increase creatine retention and muscle creatine accumulation,
likely via insulin-mediated mechanisms[15] [16].
So, if you already take creatine with a meal or a shake, you're covered.
How to take creatine
Dose: How much creatine should you take?
For most adults:
- 3-5 g daily (or ~0.1 g/kg/day) is effective[1] [2] [5]
For many people, the simplest plan is: 5 g daily, every day, with no cycling. In creatine terms, as with many other supplements, 'cycling' means
taking creatine for a set period (e.g., 4-12 weeks), then stopping for a break (e.g., 2-4 weeks) before starting again - rather than taking a
consistent daily dose year-round.
There is emerging evidence that taking a higher dose than this is beneficial, especially for brain function and cognition. I'll keep a watching
brief on studies in this area, and I'm testing it myself.
Mixing creatine at home before a walk
Creatine loading phase
Research on creatine loading
Loading is a strategy to saturate muscle creatine faster[5].
Benefits of creatine loading
You may notice benefits sooner because muscle stores rise quickly[5].
How to load creatine (simple protocol)
A common evidence-based approach:
- Loading: ~20 g/day split into 4 doses (e.g., 4 × 5 g) for 5-7 days
- Maintenance: 3-5 g/day afterward[1] [5]
If you skip loading, you can still reach saturation, it just takes longer[1] [5].
As long as you are in no particular hurry and can wait 3-4 weeks for it to take full effect, that is the way I would recommend, and the way I've
always restarted on creatine if I've not taken it for any length of time.
What happens when you start taking creatine?
You may notice:
- Better ability to repeat hard bursts[7 ‑ 10]
- Slight scale weight increase due to additional water inside the muscle (often early)[1] [2]
- Better training progression over the weeks[11] [12]
Should I take creatine every day?
Yes - daily intake is how you maintain elevated muscle stores[1] [5].
What happens when you stop taking creatine?
Muscle creatine stores gradually return towards baseline over a few weeks[11] [12].
You don't crash, but performance support fades as stores normalise.
Best time to take creatine
The evidence-based, practical answer:
- Timing matters less than consistency. Daily adherence is the key[1] [2].
- Take it whenever you remember: morning, with lunch, post-workout, any time is fine[1] [2].
- If you want to slightly optimise uptake, take it with a meal or a shake containing carbs/protein[15] [16].
How to incorporate creatine into your routine
Simple options:
- Stir into water (warm water can help dissolve)
- Mix into a smoothie or protein shake
- Add to yoghurt/porridge
- Use capsules if you dislike the texture
If creatine upsets your stomach, try:
- Smaller split doses (e.g., 2-3 g twice daily)
- Taking with food
- Avoiding heaped scoops (weigh 3-5 g)
How to select a creatine product in the UK
What actually matters when choosing creatine?
- Type: Creatine monohydrate[1] [37]
- Dose per serving: Ideally 3 g or 5 g (to make it easy to hit the evidence-based dose)[1] [5]
- Minimal extras: Avoid paying for unnecessary blends[38]
- Quality and purity: Choose reputable brands; contamination and impurities in supplements are a real concern[39]
Reading a creatine supplement label
Creapure, micronised, flavoured capsules: are these worth it?
- Creapure can be a quality signal (not more effective, but it can indicate manufacturing standards).
- Micronised often mixes better; efficacy is still essentially that of monohydrate[37].
- Flavoured: Convenient, but typically more expensive per gram.
- Capsules: Convenient but cost more per gram[38].
Safety, side effects, and misconceptions of creatine
Is creatine safe?
In healthy adults, creatine monohydrate is considered safe at recommended doses, supported by extensive research and long-term observations[1] [2].
Long-term studies in athletes report no meaningful adverse changes in clinical health markers with prolonged use[34],
and kidney-function-focused research in healthy athletes has not shown any impairment[33] .
Common side effects of creatine
- Water retention/scale weight increase early on (not fat gain)[1] [2]
- GI discomfort in some people, especially with large single doses[1] [2]
Kidney health: What people worry about versus what the data shows
- Creatine can increase creatinine (a breakdown product), which can affect some blood tests[2].
- In healthy athletes, studies show no impairment of renal function with long-term supplementation[33] [34].
- If you have known kidney disease (or are taking medications that affect the kidneys), speak to a clinician first before taking[1] [2].
Hydration, cramping, and heat illness
The claim that creatine causes dehydration or cramps doesn't hold up based on the available evidence. A systematic review found no evidence
that creatine compromises heat tolerance or body fluid balance at recommended doses[32].
Does creatine cause hair loss?
This idea largely stems from a small study in rugby players, in which the DHT:testosterone ratio changed after creatine supplementation - hair
loss itself was not measured[40].
Overall, this is not strong evidence that creatine causes hair loss, but if you're already anxious about androgenetic hair loss, it's reasonable
to be cautious and discuss it with a clinician.
Interactions
Most people don't have issues, but be mindful if you:
- Take medications that affect the kidneys
- Have medical conditions (kidney disease, bipolar disorder, etc.)
- Are pregnant/breastfeeding
Clinical caution is especially relevant when considering creatine for non-sport related reasons[1] [2] [29] [30].
Is it worth paying more for better creatine?
For most people: no.
Here's why:
- A review of creatine forms concludes that no alternative has clearly outperformed monohydrate in efficacy[37].
- A market analysis found that alternative creatine forms commonly cost more and often lack supporting evidence for their marketing claims[38].
- Head-to-head research shows that upgraded versions. such as buffered creatine and ethyl ester, don't deliver better outcomes than monohydrate[35] [36].
Walks4all takeaway
Spend your money on a quality monohydrate, use it consistently every day, and better training (plus sleep and protein).
Walks4all overall takeaway
Best creatine to take: Creatine monohydrate
Best dose: 3-5 g daily
Loading: Optional
Paying more: Rarely justified
If your goal is to feel stronger on hills, recover better from strength sessions, and maintain muscle as you age, creatine is one of the few
supplements that's consistently evidence-backed - when used correctly and paired with training[1] [11] [17 ‑ 22].
Frequently Asked Questions (FAQs) on the best types of creatine to take
What is creatine, and what does it do?
Creatine is a naturally occurring compound stored mainly in muscle tissue and also present in the brain. It helps your body rapidly
regenerate ATP during short, intense efforts, which can improve repeated high-intensity performance and training output.[1] [3] [4] [5]
What is the best type of creatine to use?
For most people, creatine monohydrate is the best option because it has the strongest evidence for effectiveness, safety, and value.
Newer, advanced forms have not consistently shown better real-world outcomes than monohydrate.[1] [2] [35 ‑ 38]
How much creatine should I take each day?
A simple, evidence-aligned daily dose is 3-5 g (or around 0.1 g/kg/day). Take it consistently to maintain elevated muscle stores.[1] [2] [5]
Do I need to do a creatine-loading phase?
No - loading is optional. Loading can saturate muscle stores faster, but daily dosing without loading still works; it just takes longer
to fully saturate.[1] [5]
When is the best time to take creatine?
The best time is whenever you will take it consistently every day. Taking it with a meal or shake can be a helpful routine and may support
retention, but timing is generally less important than daily consistency.[1] [15] [16]
Should I take creatine every day (including rest days)?
Yes. Creatine works by building and maintaining muscle creatine stores, so daily use (training and rest days) is the simplest approach
for most people.[1] [5]
How long does it take for creatine to take effect?
If you load, stores rise quickly (often within about a week). If you don't load, it typically takes 3-4 weeks of daily dosing to reach
full saturation.[1] [5]
Does creatine cause weight gain?
Creatine can cause a small increase in body weight, especially early on, mainly from additional water stored in muscle cells; it isn't
fat gain. This is more noticeable during a loading phase.[1] [2]
Is creatine harmful to your kidneys?
In healthy adults, research does not support kidney damage at recommended doses. If you have kidney disease, abnormal kidney function
tests, or take medications that affect kidney function, seek medical advice first.[1] [2] [33] [34]
Does creatine cause hair loss?
Current evidence does not show that creatine causes hair loss. One commonly cited study examined hormone markers (not hair loss itself),
and the claim hasn't been confirmed with direct hair-loss outcomes.[2] [40]
January 2026
Related reading:
 Article: Why foot health matters more as you age: Mobility, balance, fall prevention and staying independent for life
Article: Why foot health matters more as you age: Mobility, balance, fall prevention and staying independent for life
Your feet support every step you take. As we age, subtle changes in foot strength, structure, circulation, and sensation can quietly ripple outward, affecting balance, confidence, walking speed, joint health, and long‑term independence.
Published January 2026
Want to 'go deeper'?
We take evidence seriously at Walks4all. If you'd like to better understand how walking studies are designed, how results
should be interpreted, and what scientific terms mean, explore our guides on the following:
References for the best types of creatine to take
- Kreider RB, Kalman DS, Antonio J, et al. 2017. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. What the study shows: Summarises extensive evidence for effectiveness and safety across doses and populations. https://pmc.ncbi.nlm.nih.gov/articles/PMC5469049/
- Antonio J, Candow DG, Forbes SC, et al. 2021. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? What the study shows: Evidence-based answers on dosing, safety, kidneys, hydration and common myths; supports monohydrate as best-evidenced form. https://pmc.ncbi.nlm.nih.gov/articles/PMC7871530/
- Wyss M, Kaddurah-Daouk R. 2000. Creatine and creatinine metabolism. What the study shows: Explains creatine physiology, synthesis, storage and role in cellular energy metabolism. https://pubmed.ncbi.nlm.nih.gov/10893433/
- Harris RC, Söderlund K, Hultman E. 1992. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. What the study shows: Demonstrates supplementation increases muscle creatine content, supporting the mechanism of performance benefits. https://pubmed.ncbi.nlm.nih.gov/1327657/
- Hultman E, Söderlund K, Timmons JA, Cederblad G, Greenhaff PL. 1996. Muscle creatine loading in men. What the study shows: Classic loading research showing rapid increases in muscle creatine stores and informing practical loading protocols. https://pubmed.ncbi.nlm.nih.gov/8828669/
- Persky AM. 2003. Pharmacokinetics of the dietary supplement creatine. What the study shows: Reviews absorption and disposition of creatine in humans, supporting that monohydrate is effectively absorbed. https://pubmed.ncbi.nlm.nih.gov/12793840/
- Casey A, Constantin-Teodosiu D, Howell S, Hultman E, Greenhaff PL. 1996. Creatine ingestion favorably affects performance and muscle metabolism during maximal exercise in humans. What the study shows: Improved high-intensity performance and favourable muscle metabolic responses after creatine ingestion. https://pubmed.ncbi.nlm.nih.gov/8849776/
- Prevost MC, Nelson AG, Morris GS. 1997. Creatine supplementation enhances intermittent work performance. What the study shows: Creatine improved capacity to sustain repeated high-intensity intermittent efforts. https://pubmed.ncbi.nlm.nih.gov/9294877/
- Mujika I. 2000. Creatine supplementation and sprint performance in soccer players. What the study shows: Reports improvements in repeated sprint performance and reduced performance decline during intermittent tests in athletes. https://pubmed.ncbi.nlm.nih.gov/10694141/
- Balsom PD, Söderlund K, Sjödin B, Ekblom B. 1995. Skeletal muscle metabolism during short duration high-intensity exercise: influence of creatine supplementation. What the study shows: Shows creatine influences muscle metabolism during brief high-intensity exercise, supporting repeated-burst performance effects. https://pubmed.ncbi.nlm.nih.gov/7572228/
- Branch JD. 2003. Effect of creatine supplementation on body composition and performance: a meta-analysis. What the study shows: Meta-analysis finding creatine improves performance and body composition outcomes compared with placebo. https://pubmed.ncbi.nlm.nih.gov/12945830/
- Vandenberghe K, Goris M, Van Hecke P, Van Leemputte M, Vangerven L, Hespel P. 1997. Long-term creatine intake is beneficial to muscle performance during resistance training in sedentary females. What the study shows: Creatine improved strength gains in women during resistance training; stores return toward baseline after stopping. https://pubmed.ncbi.nlm.nih.gov/9390981/
- Ferguson TB. 2006. Effects of creatine monohydrate supplementation on body composition and strength in women. What the study shows: Shows creatine can improve strength and body composition measures in women during training compared with placebo. https://pubmed.ncbi.nlm.nih.gov/17194243/
- Cooke MB, Ryballa Z, Stathis CG, Cribb PJ, Hayes A. 2009. Creatine supplementation enhances muscle force recovery after eccentrically-induced muscle damage in healthy individuals. What the study shows: Improved recovery of muscle force after muscle-damaging exercise, supporting recovery benefits. https://pubmed.ncbi.nlm.nih.gov/19568173/
- Steenge GR, Simpson EJ, Greenhaff PL. 2000. Protein- and carbohydrate-induced augmentation of whole body creatine retention in humans. What the study shows: Creatine retention increased when taken with carbohydrate and/or protein plus carbohydrate. https://pubmed.ncbi.nlm.nih.gov/10956365/
- Green AL, Hultman E, Macdonald IA, Sewell DA, Greenhaff PL. 1996. Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans. What the study shows: Carbohydrate co-ingestion increased muscle creatine accumulation during supplementation. https://pubmed.ncbi.nlm.nih.gov/8944667/
- Chrusch MJ, Chilibeck PD, Chad KE, Davison KS, Burke DG. 2001. Creatine supplementation combined with resistance training in older men. What the study shows: In older men, creatine plus resistance training improved strength and body composition outcomes compared with training alone. https://pubmed.ncbi.nlm.nih.gov/11740307/
- Brose A, Parise G, Tarnopolsky MA. 2003. Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults. What the study shows: Creatine increased fat-free mass and improved strength during supervised strength training in older adults. https://pubmed.ncbi.nlm.nih.gov/12560406/
- Devries MC, Phillips SM. 2014. Creatine supplementation during resistance training in older adults-a systematic review and meta-analysis. What the study shows: Adding creatine to resistance training enhances gains in lean mass and strength in older adults. https://pubmed.ncbi.nlm.nih.gov/24576864/
- Aguiar AF. 2013. Long-term creatine supplementation improves muscular performance during resistance training in older women. What the study shows: Reports improved strength and selected functional outcomes in older women taking creatine with resistance training. https://pubmed.ncbi.nlm.nih.gov/23053133/
- Gotshalk LA. 2008. Creatine supplementation improves muscular performance in older women. What the study shows: Short-term creatine supplementation improved strength and functional performance in older women without notable adverse effects. https://pubmed.ncbi.nlm.nih.gov/17943308/
- Pinto CL. 2016. Impact of creatine supplementation in combination with resistance training on lean mass, strength, and bone mass in the elderly. What the study shows: Creatine with resistance training increased lean mass in older adults; other outcomes varied by measure and study design. https://pubmed.ncbi.nlm.nih.gov/27239423/
- Candow DG, Chilibeck PD. 2010. Potential of creatine supplementation for improving aging bone health. What the study shows: Reviews mechanisms and early evidence that creatine plus resistance training may influence bone health in ageing populations. https://pubmed.ncbi.nlm.nih.gov/20126964/
- Forbes SC. 2018. Creatine supplementation during resistance training has potential beneficial effects on properties of bone in aging adults: a systematic review. What the study shows: Systematic review of trials evaluating bone outcomes when creatine is combined with resistance training in older adults. https://pmc.ncbi.nlm.nih.gov/articles/PMC5928444/
- Gualano B. 2011. Creatine in type 2 diabetes: a randomized, double-blind, placebo-controlled trial. What the study shows: Creatine plus exercise improved glycaemic control in type 2 diabetes, suggesting synergy with training. https://pubmed.ncbi.nlm.nih.gov/20881878/
- Rae C, Digney AL, McEwan SR, Bates TC. 2003. Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. What the study shows: In a controlled crossover design, creatine improved working memory and reasoning in young adult vegetarians. https://pubmed.ncbi.nlm.nih.gov/14561278/
- McMorris T. 2006. Effect of creatine supplementation and sleep deprivation on cognitive performance, mood state, and endocrine responses. What the study shows: After sleep deprivation, creatine showed benefits for mood and selected tasks stressing executive function. https://pubmed.ncbi.nlm.nih.gov/16416332/
- Avgerinos KI, Spyrou N, Bougioukas KI, Kapogiannis D. 2018. Effects of creatine supplementation on cognitive function of healthy individuals: a systematic review of randomized controlled trials. What the study shows: Suggests possible improvements in short-term memory and reasoning, with mixed results across other domains. https://pubmed.ncbi.nlm.nih.gov/29704637/
- Lyoo IK. 2012. A randomized, double-blind placebo-controlled trial of oral creatine monohydrate augmentation in women with major depressive disorder. What the study shows: Adding creatine to SSRI treatment improved clinical response in women with major depressive disorder in an RCT. https://pubmed.ncbi.nlm.nih.gov/22864465/
- Roitman S. 2007. Creatine monohydrate in resistant depression: a preliminary study. What the study shows: Open-label pilot suggested symptom improvements while highlighting possible mania risk in bipolar depression. https://pubmed.ncbi.nlm.nih.gov/17988366/
- Hespel P. 2001. Oral creatine supplementation facilitates the rehabilitation of disuse atrophy and alters the expression of muscle myogenic factors in humans. What the study shows: Creatine supported recovery from disuse atrophy and influenced markers related to muscle regeneration during rehabilitation. https://pubmed.ncbi.nlm.nih.gov/11600695/
- Lopez RM. 2009. Does creatine supplementation hinder exercise heat tolerance or hydration status? A systematic review. What the study shows: Concludes no evidence that creatine harms heat tolerance or hydration status at recommended doses in controlled studies. https://pubmed.ncbi.nlm.nih.gov/19295968/
- Poortmans JR, Francaux M. 1999. Long-term oral creatine supplementation does not impair renal function in healthy athletes. What the study shows: Reports no detrimental effects on kidney function markers in healthy athletes using creatine long-term. https://pubmed.ncbi.nlm.nih.gov/10449011/
- Kreider RB. 2003. Long-term creatine supplementation does not significantly affect clinical markers of health in athletes. What the study shows: Prolonged creatine use did not adversely affect a broad panel of clinical health markers in athletes. https://pubmed.ncbi.nlm.nih.gov/12701816/
- Jagim AR. 2012. A buffered form of creatine does not promote greater changes in muscle creatine content, body composition, or training adaptations than creatine monohydrate. What the study shows: Buffered creatine was not superior to monohydrate for key outcomes in a controlled training study. https://pubmed.ncbi.nlm.nih.gov/22971354/
- Spillane M. 2009. The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels. What the study shows: Ethyl ester did not outperform monohydrate and was less effective at raising muscle creatine in this training study. https://pubmed.ncbi.nlm.nih.gov/19228401/
- Kreider RB. 2022. Bioavailability, efficacy, safety, and regulatory status of creatine and creatine forms intended for sports nutrition. What the study shows: Review of creatine forms concluding monohydrate remains most proven, with no consistent superiority from novel forms. https://pmc.ncbi.nlm.nih.gov/articles/PMC8912867/
- Escalante G. 2022. Analysis of the efficacy, safety, and cost of alternative forms of creatine sold as dietary supplements. What the study shows: Finds many alternative forms have limited evidence and are typically more expensive per gram than monohydrate. https://pmc.ncbi.nlm.nih.gov/articles/PMC9761713/
- Moret S, Prevarin A, Tubaro F. 2011. Levels of creatine, organic contaminants and heavy metals in creatine dietary supplements. What the study shows: Market analysis found variability in content and detectable contaminants in some samples, supporting reputable sourcing. https://doi.org/10.1016/j.foodchem.2010.12.028
- van der Merwe J. 2009. Three weeks of creatine monohydrate supplementation affects dihydrotestosterone to testosterone ratio in college-aged rugby players. What the study shows: Reports changes in androgen measures; hair loss outcomes were not directly measured. https://pubmed.ncbi.nlm.nih.gov/19741313/